



Note: This post is a blend of theory and insights. Stay with me till the end. :-)
I know rhexis is a touchy topic. Quite understandable so given the fact that in most Indian OTs, we are stuck with HPMC as the only OVD available and rhexis forceps are not provided as standard. So let’s dive straight into it.
You might have heard the phrase, ‘the capsule is so elastic’.
Truth be told, the lens capsule is a Type IV collagen tissue (the thickest basement membrane in our body). It is the forces that act on the capsule due to which it behaves like an elastic tissue. The aim of capsulorhexis should be to minimise these forces whenever possible and prevent accumulation of undue potential energy in it so as to facilitate a smooth, predictable rhexis of desired size. Some of the forces acting on the anterior lens capsule are:
Intra-lenticular pressure
Intra-cameral pressure
Zonular tension
Does vitreous upthrust affect rhexis?
Yes and no. Although a high vitreous upthrust does not act directly on the anterior lens capsule, its effects on lenticular pressure, zonular stress and the anterior chamber can contribute in making rhexis an unpredictable affair. A generous massage after a peribulbar block to attain an IOP in low teens is very important to counter this where necessary. Try the Pinky ball. You may consider pre-op mannitol (MOA: It sucks water out of the vitreous) if required. Avoid mannitol in cases with high BP as it increases the risk of cerebral edema.
What exactly does trypan blue do?
Trypan blue 0.6mg/ml (0.06%) is an Azo dye which acts as a vital stain (stains dead tissue). It is acidic in nature but is pH adjusted for intra-cameral use (US-FDA approved in 2004). It stains only the basement membrane and not the underlying cortex nor the internal lens epithelial cells (cells that undergo hyperplasia and change to spindle shaped myofibroblast-like cells that later form posterior capsular opacity/after cataract). This explains as to why it is preferred in cases of poor fundal glow (where the only contrast available is a blue capsule against white cortex) or in cases with posterior segment pathologies such as RD or VH. This is also the reason why fluorescein fails as a substitute as it stains the underlying cortex as well, therefore taking away the contrast advantage. ICG can be used but trypan blue simply stains better.
Dick et al demonstrated the effects of Trypan blue on the biomechanical properties of lens capsule (i.e. reduction in elasticity leading to an increase in the stiffness of lens capsule and DM). Trypan Blue can cause leopard spot staining pattern if left in contact with the endothelium for too long. So save the DM and the endothelium and inject a single large air bubble in AC, leave the dye for about 10-15 secs (maybe 30-40 secs for harder grades) and wash well. Trypan blue also has some role in preventing PCO by killing lens epithelial cells. But it needs to be injected inside the bag for this.
Continuous Curvilinear Capsulorhexis (CCC) was independently developed by Dr Howard Gimbel and Thomas Neuhann. CCC changed the game forever and made modern day Phacoemulsification very safe with respect to complications such as a drop or IOL decentration and also allows for a confident sulcus fixation with optic capture.
Here are some elementary physics concepts behind the CCC.
Stress is the force divided by the cross sectional area where the force is being applied.
Strain is the change in length of a deformed material divided by its original length.
Increased stress will deform an elastic tissue which, resultantly, will experience strain. A material is permanently deformed if the strain experienced increases beyond its elastic limit. Any further stress will tear the tissue. This is the breaking point. Trypan blue makes the capsule fragile, reducing its ability to deform extensively (i.e. breaking point is reached faster) and this results in easy tearing of the capsule.
Two terms to know for the uninitiated. Rip and Shear. Shear does most of the job. Rip saves ass when most needed.
Shear does most of the job. Rip saves ass when most needed.
There is a misconception that using a cystitome gives you a shear whereas a rhexis forcep will give you a rip. But this is not true. Both cystitome and forceps can give you either, but a rip should be avoided with a capsulotomy because in a rip, the forces (/stress) are spread over a larger area which can result in a sudden uncontrolled runout even though you may be pulling radially towards the centre. Shear offers decent control and speed until the forces get unbalanced and the rhexis started to go out. An expert surgeon using rhexis forceps will begin with a shear and proceed for about 2-3 clock hours and then pivot in a way that the forces are now coverted into a rip for about 1-2 clock hours and then stop to regrasp. This manoeuvre of grasp-shear-rip-regrasp is performed about 4-5 times to complete the rhexis in its entirety.
When leveraging a shear for normal rhexis with a rhexis forcep, hold about 2 clock hours away from the point of shear. Holding too close can change the direction of vectors creating a new arc. If rip is being used as a rescue manoeuvre, hold as close as possible to the tearing edge (watch the second video).
It is important to keep the torn region spread out over the lens surface as a wrinkled flap will undesirably convert a shear into a rip and cause the rhexis to run out or make it unreasonably small.
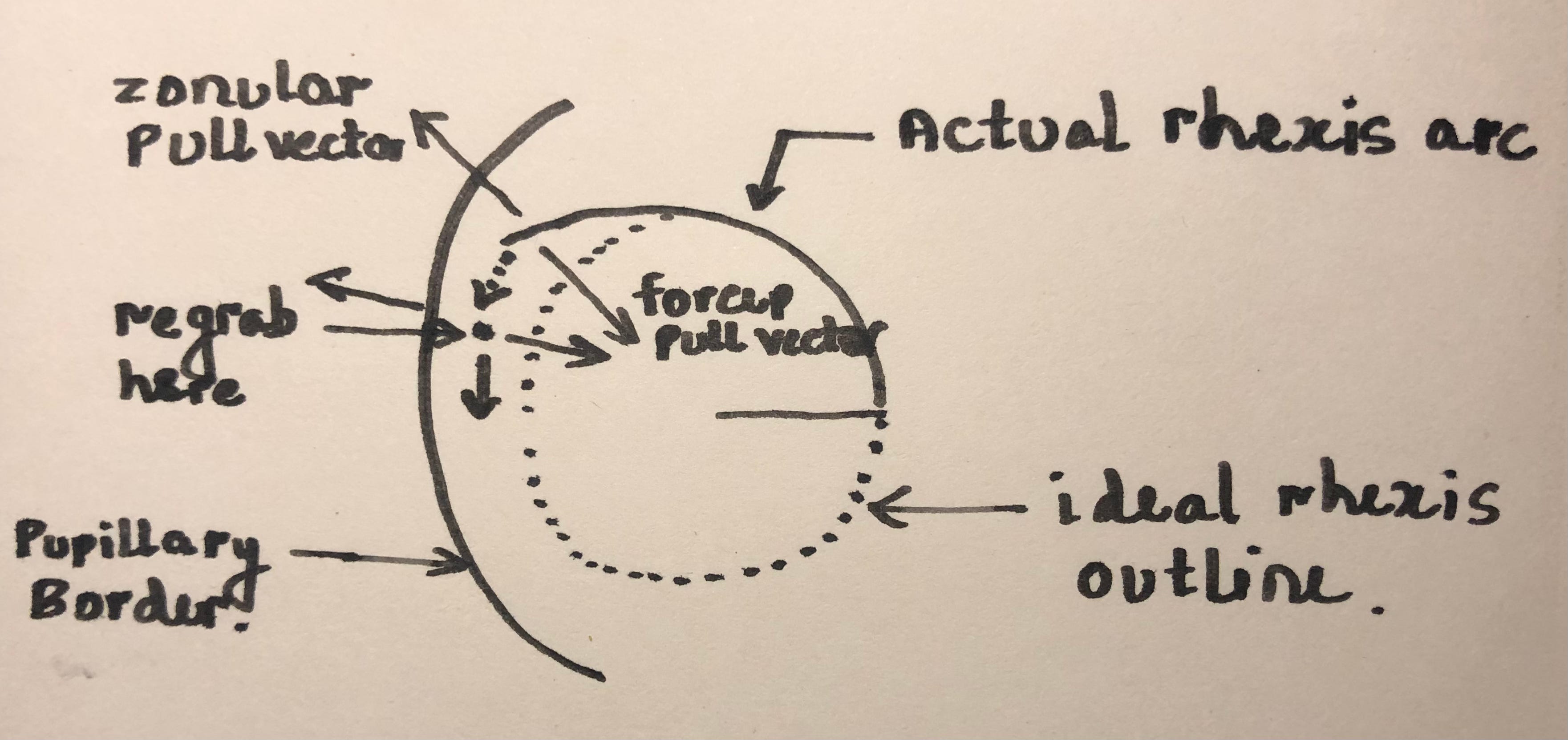
A shear more or less propagates in the direction you are pushing/tearing the capsule in until the forces get unbalanced (first video where the rhexis ran out after forces got unbalanced). On the other hand, in a successfully implemented rip, the tear should propagate in a direction that will bisect the vectors of the two opposing forces (zonular pull outwards and instrument pull inwards). See image below.
What to do if the rhexis extends?
For most cases falling in the normal spectrum of nuclear grades, slight extension beyond the pupil is acceptable and is almost always inconsequential if managed correctly. Quick pull manoevre may be tried under an experienced surgeon’s observation. Remember that a poorly executed 'quick pull’ can cause more harm than a extended rhexis left alone. Anterior zonules are attached much more anteriorly than the equator and a extended rhexis flap (unless unnecessarily disturbed) should stop here. At this point, just grab a pair of scissors (vannas, rhexis scissors or intravitreal scissors), give a fresh cut at a point proximal to the point of ‘run out’ and complete the rhexis. Be very gentle with hydro procedures and nucleus rotation. You can then reduce bottle height, maintain AC stability (till the last step i.e. hydration of wounds), reduce aspiration rate, tumble the nucleus out of the bag early to successfully complete Phaco and put a lens in the bag. Place the haptics perpendicular to the site of extension. A Phaco mindset is imperative in such situations to control your desire to convert to SICS/ECCE.
A Phaco mindset is imperative in such situations to control your desire to convert to SICS/ECCE.
References:
Frederick “Fritz” T. Fraunfelder MD, Frederick “Rick” W. Fraunfelder MD, MBA, in Drug-Induced Ocular Side Effects (Eighth Edition), 2021
Singh, A., Sarodia, U., Brown, L. et al. A histological analysis of lens capsules stained with trypan blue for capsulorrhexis in phacoemulsification cataract surgery. Eye 17, 567–570 (2003). https://doi.org/10.1038/sj.eye.6700440
Dick HB, Aliyeva SE, Hengerer F. Effect of trypan blue on the elasticity of the human anterior lens capsule. J Cataract Refract Surg. 2008 Aug;34(8):1367-73. doi: 10.1016/j.jcrs.2008.03.041. PMID: 18655989.
S. Sinumol, P.S. Jayalakshmy, Thulaseedharan Sreedharan, Mallika Odamparambil Unni, Smita Narayan, N. Sujatha, Effect of intraoperative trypan blue on lens epithelial cells: Histomorphological analysis, Saudi Journal of Ophthalmology, Volume 33, Issue 1, 2019, Pages 18-23, ISSN 1319-4534, https://doi.org/10.1016/j.sjopt.2018.12.006.
ophed.com Section 5 Physics of Capsuloprhexis (Siebel)